Latest articles
274 articles HRT
HRTHow to Get HRT Online: The 2026 Guide
Telehealth has rewritten access to hormone replacement therapy. Step-by-step process, who qualifies, what to expect, and how the right service prevents wasted months on the wrong dose.
 HRT
HRTHRT Cost Without Insurance: The 2026 Guide
What hormone replacement therapy actually costs in 2026, without insurance, without hidden fees, and without overpaying for the same compound. A line-by-line breakdown.
 Telehealth
TelehealthBrand vs Compounded GLP-1s and TRT: What's Actually Different
Compounded medications cost less and offer dosing flexibility. Brand-name carry maximum regulatory rigor. The honest comparison.
 TRT
TRTHow to Inject Testosterone: Subcutaneous vs. Intramuscular
Step-by-step guide. Needle sizes, injection sites, technique, and safety.
 HRT
HRTCan Women Take Testosterone? How Much Is Safe?
Yes, and increasingly part of comprehensive HRT. Female doses are 1/10th to 1/20th of male; benefits are real.
 TRT
TRTThe Complete Guide to TRT in 2026
Testosterone replacement therapy, demystified. Symptoms, lab ranges, dosing protocols, and how telehealth has changed access.
 HRT
HRTWhen to Start HRT: The Symptoms Window for Women
The "wait until you've stopped getting periods" advice is outdated. Why earlier HRT often produces better cardiovascular and bone outcomes.
Enclomiphene vs. TRT: Which Is Right for You?
Two paths to raising testosterone, one preserves fertility, one doesn't. Here's how to choose.
 Telehealth
TelehealthIs Telehealth TRT Legitimate?
Yes, when the clinic actually does the work. Twelve red flags and twelve green flags.
 Telehealth
TelehealthThe Complete Guide to Online Hormone Therapy
How online hormone therapy works in 2026. Evaluation, prescribing, delivery, safety, costs.
 TRT
TRTFree vs Total Testosterone: The Binding Biology
Total testosterone is the headline number, but free T is what tissues actually access. Understanding both is essential for accurate TRT decisions.
 TRT
TRTSubcutaneous vs Intramuscular Testosterone Injections
SubQ is the modern default, equivalent absorption, smoother kinetics, smaller needles, easier self-administration.
 TRT
TRTTRT Pellets vs Injections vs Cream
Each delivery route has tradeoffs. Why subcutaneous injections are the modern default for most patients.
 Telehealth
TelehealthHow to Choose a Telehealth Provider: Red Flags and Green Flags
Twelve questions that separate legitimate medicine from prescription mills.
 Telehealth
TelehealthTelehealth Weight Loss: How It Actually Works
Complete guide to telehealth weight loss. How online GLP-1 prescriptions work and how to evaluate clinics.
 Training
TrainingEating in a Surplus: How Much Is Actually Needed for Muscle
"Eat big to get big" is mostly wrong. The optimal surplus is much smaller than bro-science suggests.
 Telehealth
TelehealthWhat Is Compounded Medication? (10x Better Than Gray Market)
Compounded medications explained. Legal, FDA-regulated, safe, and completely different from research peptide sites.
 Weight Loss
Weight LossTirzepatide vs Mounjaro vs Zepbound: What's Actually Different
Same molecule. Different brand routes. Plus where compounded tirzepatide fits in.
 Weight Loss
Weight LossGLP-1 vs. Bariatric Surgery: The Comparison in 2026
GLP-1 therapy has produced weight losses approaching bariatric surgery for some patients, without the surgical risk. Here's the honest comparison in 2026.
 Lifestyle
LifestyleAlcohol's Real Cost: A Marker-by-Marker Breakdown
What alcohol does to testosterone, estradiol, sleep, lipids, ApoB, inflammation, and breast cancer risk. The objective evidence.
 Nutrition
NutritionThe Protein Question: How Much Do You Actually Need?
The federal RDA is 2x too low for active adults. The leucine threshold, optimal amounts by goal, and why older adults need more, not less.
 TRT
TRTShould I Take HCG With My TRT? A Decision Guide
The simple framework for whether to add HCG. Fertility, testicular volume, hormonal completeness, what matters for you.
 TRT
TRT10 Signs of Low Testosterone You Shouldn't Ignore
Low energy, brain fog, weak erections, stubborn weight gain. The pattern of hypogonadism, and when to get tested.
 Weight Loss
Weight LossWhat Is Semaglutide? The Complete Overview
How the drug that started it all works, why it's effective, and what to expect if you consider it.
 HRT
HRTPerimenopause vs Menopause: What's the Difference?
Perimenopause is the multi-year transition; menopause is a single day. Different physiology, different treatment.
 Weight Loss
Weight LossGLP-1 Side Effects: The Honest Guide to Managing Them
Nausea, constipation, muscle loss, "Ozempic face", what's real, what's hype, and how to prevent the problems that are avoidable.
 Enclomiphene
EnclomipheneHow fast does enclomiphene raise testosterone?
Total T rises 2-4 weeks, peaks at 8-12. 200-400 ng/dL above baseline. Fertility preserved, unlike TRT.
 Lab Testing
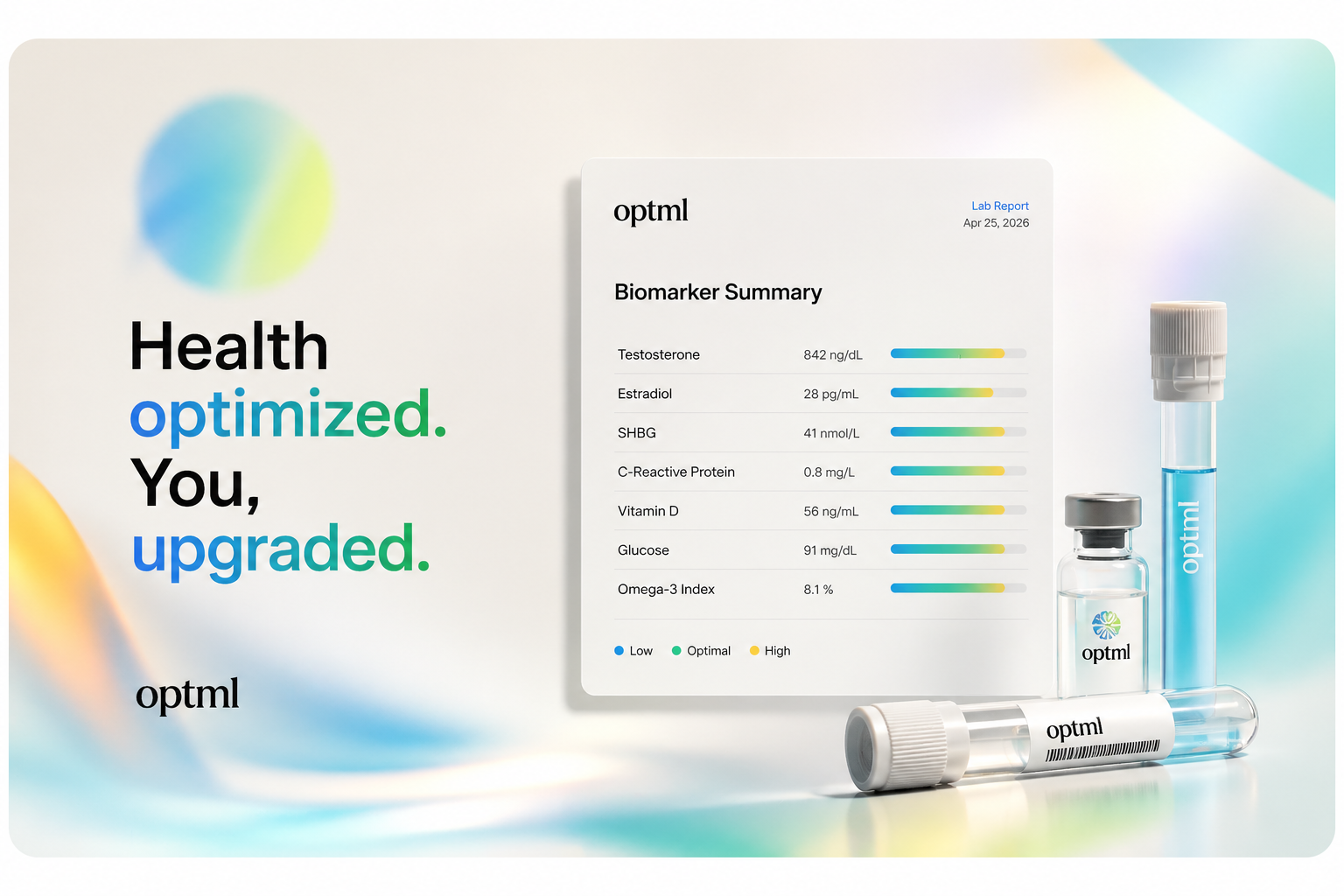
Lab TestingThe Complete Guide to Optimized Blood Panels
Which biomarkers actually predict health, what your doctor probably isn't ordering, and how to interpret results.
 Sermorelin
SermorelinIs Sermorelin Worth It? An Honest 2026 Breakdown
Sermorelin gets either over-hyped or dismissed entirely. The truth is in the middle, it's worth it for a specific patient profile and not worth it for others. Here's the breakdown.
 Longevity
LongevityWhat Is NAD+? The Cellular Energy Molecule Explained
Why NAD+ is the metabolic cofactor everyone's talking about, and what precursors (NR, NMN, IV) actually do.
 Weight Loss
Weight LossHow Long Does Tirzepatide Stay in Your System?
5-day half-life. ~25-day full clearance. Practical implications for missed doses, surgery, and stopping.
 TRT
TRTYour First 30 Days on TRT: What Actually Happens
The honest, realistic walkthrough of starting TRT. What you'll feel week by week.
 Longevity
LongevityBiological Age vs. Chronological Age: How to Reverse It
What biological age is, how it's measured (GrimAge, PhenoAge), and the interventions proven to reverse it.
 Longevity
LongevityAMPK vs mTOR: The Cellular Energy-Growth Balance
AMPK is the cellular fuel gauge; mTOR is the growth signal. The balance between them determines whether cells age through growth or through stress resistance.
 TRT
TRTThe Real Side Effects of TRT (Honest Edition)
Common, monitorable, rare, and resolved-by-data. The complete honest accounting of TRT side effects.
 Training
TrainingBulking and Cutting vs Recomposition: Which Wins?
Two strategies, different populations. The honest decision framework for which fits your situation.
 Training
TrainingTraining for Fat Loss vs Training for Muscle: The Real Differences
The "fat loss workout" myth, what actually changes in a deficit, and why most cutting programs sabotage muscle preservation.
 Longevity
LongevityIs NAD+ Worth It? The Honest Take
Plausible, popular, partially evidenced. A refined adjunct, not a foundation. Where it fits and where it doesn't.
 HRT
HRTHRT Side Effects, Honestly: What's Real, What's Overstated
Twenty years of fear shaped women's medicine. The data has changed. What's actually risky, what's overstated, and what modern HRT looks like in 2026.
 Weight Loss
Weight LossThe Complete Semaglutide Dosing Guide
Starting doses, titration schedules, maintenance, and what to do when side effects or plateaus show up.
 Nutrition
NutritionMediterranean Diet vs Keto vs High-Protein: Which Wins?
Each has strengths. The honest comparison and the hybrid that beats them all for most adults.
 Nutrition
NutritionTime-Restricted Eating: Real vs. Marketing
The mechanism is mostly caloric reduction, not metabolic magic. Useful tool, when it fits your life.
 TRT
TRTHCG Monotherapy: Raising Testosterone Without TRT
For men with secondary hypogonadism wanting elevation without exogenous testosterone, HCG monotherapy is a legitimate alternative.
 Lab Panels
Lab PanelsOptimal vs Normal Lab Ranges: The Gap That Matters
Reference ranges describe what's common, not what's healthy. Where the gap lives, and why so many adults feel terrible with "normal" labs.
 Weight Loss
Weight LossSemaglutide for PCOS: How GLP-1s Are Changing Treatment
PCOS is driven by insulin resistance, exactly what GLP-1s treat. Here's what the research shows.
 Labs
LabsFasting Glucose vs CGM: What Each Captures
Fasting glucose is one moment. CGM is the full day. Both are useful, they capture different things.
 TRT
TRTTestosterone Levels by Age: Chart + What's Normal
Complete age-by-age breakdown. Normal ranges, optimal ranges, what's low.
 TRT
TRTDo I Have Low Testosterone? 15-Question Checklist
Interactive symptom quiz. Score your symptoms and learn whether to get tested.
 TRT
TRTTRT for Men with Type 2 Diabetes: What the Research Shows
Low T and T2D form a vicious cycle. TRT can improve insulin sensitivity, reduce visceral fat, lower A1C.
 TRT
TRTTestosterone and Visceral Fat: The Bidirectional Relationship
Visceral fat and low testosterone create a self-reinforcing loop. Each promotes the other. Breaking the cycle often requires direct intervention.
 TRT
TRTWhy Free Testosterone Matters More Than Total
Total T is the headline. Free T is what you actually feel. Why two men with identical total T can be functionally hypogonadal or thriving, depending on SHBG.
 TRT
TRTDoes TRT Cause Hair Loss?
It accelerates pattern baldness in genetically susceptible men, but doesn't create new susceptibility. The data and the prevention strategies.
 TRT
TRTTRT in Young Men Under 30: When It Makes Sense
Most young men with low T have a fixable cause. Default-to-TRT is often wrong sequence. Address the cause first.
 TRT
TRTHCG on TRT: Why Most Men Should Consider It
Preserving fertility, testicular function, and intratesticular testosterone. Why HCG belongs on most TRT protocols.
 TRT
TRTWhen to Cycle Off TRT (Or Not)
The "cycle off" framing comes from steroid culture, not therapeutic medicine. When discontinuation makes sense, when it doesn't, and what restart looks like.
 TRT
TRTHematocrit Management on TRT: The Polycythemia Question
The most common monitorable side effect, and the most over-feared. When it actually matters, when it doesn't, and how to manage it.
 TRT
TRTPSA on TRT: What's Normal and What's Not
Modest initial rise expected. The saturation model has reshaped the prostate cancer fears that historically held the field back.
 TRT
TRTEstradiol Management on TRT: The Goldilocks Zone
Too low destroys joints, libido, and bones. Too high causes water retention and gynecomastia. The narrow optimal window most physicians get wrong.
 TRT
TRTAnastrozole on TRT: When (and When Not) to Use It
Anastrozole is over-prescribed. The clear framework for when it's actually appropriate, and when it harms.
 TRT
TRTTestosterone and Cardiovascular Outcomes: The TRAVERSE Resolution
The TRAVERSE trial settled a decade of controversy: TRT in men with low T and cardiovascular risk does not increase cardiovascular events. The data and what it changes.
 TRT
TRTTestosterone and Mood: When Low T Looks Like Depression
Many men labeled as depressed have undiagnosed low testosterone. The symptom overlap is substantial, and treating the right cause matters.
 TRT
TRTTestosterone and Cognition: What the Research Shows
Testosterone affects far more than muscle and libido. Brain receptors are dense in memory and executive function regions, and clinical evidence supports cognitive benefit from optimization.
 TRT
TRTTestosterone and Sleep Architecture
Sleep and testosterone reinforce each other. Poor sleep suppresses T; low T degrades sleep. The bidirectional loop and how TRT changes it.
 TRT
TRTTestosterone and Anxiety: The Modulator
Anxiety in middle-aged men is often dismissed as life stress. Sometimes it's hormonal, and treatable.
 TRT
TRTTestosterone and Bone Density: The Mechanism
Men with low T have higher osteoporosis rates than commonly recognized. The mechanism is multi-factorial, and TRT can reverse the trajectory.
 TRT
TRTTestosterone and Insulin Sensitivity
Low T and insulin resistance are tightly linked. Treating one tends to improve the other, and combined treatment is often required.
 TRT
TRTTestosterone and Dopamine: The Drive Connection
The lack of drive that men with low T describe isn't laziness. It's a measurable change in dopamine signaling.
 TRT
TRTTestosterone and Immune Function: The Modulator
Testosterone modulates immune function. Too low or too high produces different problems. The biology of why men's immune systems differ from women's.
 TRT
TRTTestosterone and the Vascular Endothelium
Testosterone affects vascular function in nuanced ways. Adequate levels support endothelial health and nitric oxide function, drivers of cardiovascular outcomes.
 TRT
TRTTestosterone and Red Blood Cells: Why Hematocrit Matters
Testosterone stimulates red blood cell production. Most TRT patients see modest hematocrit rise; some need active management.
 HRT
HRTShould Women in Their 30s Be on HRT?
Most don't need full HRT yet, but late-30s progesterone deficiency is common and underdiagnosed. The targeted answer.
 TRT
TRTWhy Your Doctor Won't Prescribe TRT (Even When You Need It)
The structural reasons, outdated training, lab range conventions, time constraints, reimbursement. And what to do.
 HRT
HRTHRT and Migraines: Friend or Foe?
Steady transdermal estradiol usually helps. Oral or cyclical can hurt. The difference is in the details.
 TRT
TRTWhy Am I Gaining Weight on TRT?
The first 4-8 weeks are mostly water and glycogen, not fat. The body composition picture takes months to settle.
 TRT
TRTBest Time of Day to Take TRT Injections
For most TRT protocols, time of day doesn't matter. Consistency does. Here's why.
 TRT
TRTWhat ChatGPT Gets Wrong About TRT
AI assistants still repeat outdated TRT myths. The current evidence has moved past several of them.
 TRT
TRTEnclomiphene for Fertility: What It Actually Does
Raises testosterone via the natural HPG axis, preserving fertility instead of suppressing it.
 HRT
HRTHRT and Cardiovascular Health: The Surprising Story
Started in the window of opportunity, HRT improves arterial elasticity, lipids, and reduces all-cause mortality. The 20-year follow-up data.
 HRT
HRTHRT for Bone Density: Preventing Osteoporosis Before It Starts
Estrogen is the most powerful tool for women's bone health, but only if you start before the loss accelerates.
 TRT
TRTFertility on TRT: How to Protect It
Standard TRT shuts down sperm production within 6 months. With HCG, enclomiphene, or sperm banking, fertility is preservable. The complete guide.
 TRT
TRTTRT for Longevity: The Healthspan Argument
The 2024 TRAVERSE trial repositioned TRT as a longevity tool. Muscle, bone, metabolic, and mortality benefits with appropriate use.
 TRT
TRTTRT and Estrogen: Do You Need an Aromatase Inhibitor?
Modern evidence says most men should avoid AIs. When estrogen management matters, and when it doesn't.
 HRT
HRTTestosterone for Women: The Overlooked Hormone
Women make testosterone too. Low-dose therapy is transformative for libido, mood, muscle, and energy in the right candidates.
 HRT
HRTHRT for Women: A 2026 Guide to Perimenopause and Menopause
The evidence-based truth about hormone replacement therapy for women, estrogen, progesterone, testosterone, and risk vs. reward.
 Weight Loss
Weight LossHow GLP-1 Medications Actually Work
The mechanism of action behind the weight-loss revolution, and why it's not just "about eating less."
 Weight Loss
Weight LossGLP-1s in Perimenopause: Weight Loss for Women 40+
Why GLP-1s are uniquely effective for perimenopausal women, and how to combine with HRT.
 Weight Loss
Weight LossWhy Is My GLP-1 Not Working Anymore?
Plateaus are rarely "the drug stopped." Six common causes, and the protocol to break through.
 Weight Loss
Weight LossWhat Happens When You Stop Semaglutide?
STEP-4 showed two-thirds of weight returns at 12 months without a maintenance plan. The protocol that keeps the results.
 Weight Loss
Weight LossGLP-1 and Visceral Fat: Why It Drops Disproportionately
Visceral fat is the dangerous kind. GLP-1 therapy reduces it disproportionately to total weight loss, explaining a chunk of the cardiovascular and metabolic benefits.
 Weight Loss
Weight LossThe Muscle Preservation Playbook on GLP-1 Therapy
Step-by-step protocol for preserving muscle through aggressive weight loss on GLP-1 therapy. Specific numbers, specific sequences.
 Weight Loss
Weight LossGLP-1 and the PCOS Metabolic Phenotype
PCOS is increasingly understood as a metabolic disorder for many patients. GLP-1 therapy treats the root rather than the surface, and the cascade of improvements is often dramatic.
 Weight Loss
Weight LossGLP-1 and Sleep Apnea: The SURMOUNT-OSA Findings
The SURMOUNT-OSA trial showed tirzepatide cut apnea-hypopnea index roughly in half. The mechanism, the implications, and why this matters even for patients without diagnosed apnea.
 Weight Loss
Weight LossGLP-1 in the Brain: Mood, Reward, and Cognition
GLP-1 receptors are expressed throughout the brain. Understanding the central effects explains why these drugs change cravings, mood, and possibly cognition.
 Weight Loss
Weight LossGLP-1 and Alcohol Use: The Cravings Reduction
Patients on semaglutide and tirzepatide consistently report drinking less. The mesolimbic reward circuit dampening is the mechanism.
 Weight Loss
Weight LossGLP-1 and Fertility: What the Data Shows
Many patients started on GLP-1 therapy for weight loss become pregnant unexpectedly. The mechanism: restored ovulation. Here's what's known and what's not.
 Weight Loss
Weight LossGLP-1 and Cardiovascular Outcomes: The Trial Data
Cardiovascular outcome trials of GLP-1 agonists have changed how we think about these medications. Heart disease event rates drop by ~14-20%, and the mechanism is much more than weight loss.
 Weight Loss
Weight LossGLP-1 and Menopause Weight: Why It Works When Diet Doesn't
Many women find menopausal weight gain resistant to the strategies that worked in their 30s and 40s. The hormonal shift requires hormonal-aware treatment.
 Weight Loss
Weight LossGLP-1 and Fatty Liver: NAFLD/MASH Resolution
Non-alcoholic fatty liver disease (now MASLD/MASH) is the most common chronic liver disease worldwide. GLP-1 therapy is becoming a primary treatment.
 Weight Loss
Weight LossGLP-1 and Joint Pain: How Inflammation Reduction Helps
Patients on GLP-1 therapy commonly report less knee, hip, and back pain. Some of that is mechanical, less weight on joints. Some is anti-inflammatory.
 Weight Loss
Weight LossGLP-1 and Gut Motility: Beyond Slowed Stomach Emptying
Slowed gastric emptying is the most-discussed gut effect, but GLP-1 affects motility from stomach to colon. The full picture explains every GI side effect.
 Weight Loss
Weight LossGLP-1 and Skin: Ozempic Face, Acne, and Collagen
Skin changes on GLP-1 therapy fall in two camps: structural changes from rapid fat loss ("Ozempic face") and inflammatory improvements (acne, redness). Both have explanations.
 Weight Loss
Weight LossGLP-1 and Cancer Risk: What the Literature Actually Shows
Cancer concerns dominated early GLP-1 discourse. Ten years later, what does the data actually show, about thyroid, pancreas, colon, breast, and overall cancer risk?
 Weight Loss
Weight LossGLP-1 and Kidney Protection: The FLOW Trial and Mechanism
Diabetic kidney disease is the leading cause of kidney failure. GLP-1 therapy slows its progression substantially, through inflammation reduction, blood pressure improvement, and direct renal effe...
 Weight Loss
Weight LossGLP-1 and Dopamine: The Reward System Reset
Dopamine drives the wanting that turns food cues into food searches. GLP-1 therapy dampens that wanting at the receptor level.
 Weight Loss
Weight LossGLP-1 and Alzheimer's Disease: The Active Trials
GLP-1 receptors are expressed in the hippocampus. Brain insulin resistance is implicated in Alzheimer's. Multiple large trials are testing the connection.
 Weight Loss
Weight LossGLP-1 and Bone Health: Managing Osteoporosis Risk
Rapid weight loss reduces bone density. The mechanism, the trial data, and how to protect bone during GLP-1 therapy.
 Weight Loss
Weight LossGLP-1 and Insulin Sensitivity Beyond Weight Loss
GLP-1 therapy improves insulin sensitivity through multiple mechanisms, only some of which are downstream of weight loss. Here's what's direct and what's indirect.
 Weight Loss
Weight LossGLP-1 Dose-Response: Why More Isn't Always Better
Higher GLP-1 doses produce more weight loss, up to a point. Beyond that, side effects accumulate without proportional benefit. Finding the personal optimal dose matters.
 Weight Loss
Weight LossGLP-1 + Resistance Training: The Synergy Playbook
Patients on GLP-1 therapy who resistance train end up with dramatically different body composition than those who don't. Same scale weight, very different bodies.
 Weight Loss
Weight LossGLP-1 and ADHD-Type Eating Patterns
Adults with ADHD often have characteristic eating patterns driven by dopamine biology. The same biology GLP-1 therapy modulates.
 Weight Loss
Weight LossCan Tirzepatide Help With Sleep Apnea?
SURMOUNT-OSA cut apneas in half. The first major pharmaceutical advance in OSA management in decades.
 Weight Loss
Weight LossGLP-1s and Muscle Preservation: How to Lose Fat Without Losing Lean Mass
The data on muscle loss with GLP-1s, and the protein-training-hormone protocol that closes the gap.
 Nutrition
NutritionAlcohol on TRT and GLP-1s: What You Need to Know
How alcohol interacts with TRT, semaglutide, tirzepatide, and HRT. How much is actually okay.
 Fitness
FitnessThe Menopause Exercise Guide: Strength Training Beats Cardio
Why heavy lifting, not cardio or HIIT, is the right prescription for women 40+. The real exercise framework for menopause.
 HRT
HRTEstrogen Levels by Age: Women's Chart + What's Normal
Complete estradiol chart through reproductive years, perimenopause, and menopause.
 TRT
TRTThe Real Reasons Men Get Belly Fat After 35
Belly fat after 35 isn't a willpower issue, it's a hormonal feedback loop. Breaking it requires hitting multiple levers at once.
 TRT
TRTWhat Does Low Estrogen Feel Like in a Man?
Joint pain, crashed libido, dry eyes, depressed mood. Why crushing estradiol on TRT does more harm than good.
TRTEstradiol in Men: The Protective Role We Underappreciate
Estradiol gets a bad rap in men's health. The data says it's essential, for bone, brain, joints, and cardiovascular function. Why aggressive suppression is usually wrong.
 HRT
HRTEstradiol and the Female Brain
The brain has more estrogen receptors per gram than the uterus. Declining estradiol through perimenopause produces measurable cognitive, mood, and neuroprotective consequences.
 HRT
HRTEstradiol and Bone: The Master Bone Hormone
Estradiol is the master bone hormone, in women and in men. The biology explains why menopause produces accelerated bone loss and why HRT prevents it.
 HRT
HRTEstradiol and Skin: The Collagen Connection
Skin loses collagen rapidly after menopause. The driver is estradiol decline. HRT slows the loss measurably.
 HRT
HRTEstradiol and Cardiovascular Health
Women's cardiovascular risk catches up to men's after menopause. The driver is estradiol loss, and HRT timing matters for cardiovascular outcomes.
 HRT
HRTProgesterone, GABA, and Sleep: The Calming Connection
Progesterone is more than a reproductive hormone. Its metabolite allopregnanolone is one of the body's most potent natural GABA enhancers.
 HRT
HRTProgesterone and Anxiety: The Anxiolytic Hormone
Anxiety in perimenopause is often driven by declining progesterone. The GABA mechanism explains why, and why bioidentical progesterone helps.
 HRT
HRTProgesterone and Breast Tissue: The Bioidentical Distinction
The breast cancer concerns about HRT came from synthetic progestins. Bioidentical progesterone has a different profile, and the distinction matters for modern HRT.
 HRT
HRTWhy Your Period Is Suddenly Heavier in Your 40s
The perimenopausal anovulation pattern, and the targeted treatment that resolves most cases within 2-3 cycles.
 HRT
HRTVaginal Estrogen: The Most Underused Tool in Women's Medicine
Resolves urinary urgency, painful intercourse, and recurrent UTIs in postmenopausal women, even safe for many breast cancer survivors.
 HRT
HRTAMH Testing: What Your Ovarian Reserve Number Means
AMH measures reserve, not quality. Useful for fertility planning and rough menopause prediction, commonly misinterpreted.
 HRT
HRTThe PCOS Playbook in 2026
PCOS is fundamentally an insulin-resistance disorder. The modern playbook addresses the root with GLP-1s, inositol, training, and sleep.
 HRT
HRTEstrogen Dominance: Real Phenomenon or Marketing Myth?
The concept is half-real, half-marketing. What's clinically valid, where it gets oversold, and how to actually evaluate yours.
 HRT
HRTThe Female Athlete Triad and RED-S: How to Recognize and Avoid It
Active women under-eating relative to training develop predictable hormonal, menstrual, and bone consequences. How to identify and recover.
 HRT
HRTThe Postmenopausal Body Composition Reset
The postmenopausal body shift isn't fixed by trying harder at what worked at 35. Modern protocols and the integrated approach.
 TRT
TRTDHEA Supplementation for Men: When It Makes Sense
DHEA-S declines 80% from age 25 to 75. When supplementation actually helps, dosing, and how it interacts with TRT.
 HRT
HRTPelvic Floor and Hormones: The Connection Most Women Miss
Pelvic floor problems are often blamed on aging or childbirth. The bigger driver is usually estrogen decline, and the fix involves more than kegels.
 HRT
HRTPostpartum Hormone Rebuilding: The First 12 Months
The hormonal crash after birth is the steepest cliff in human physiology. The labs and protocol that help women recover faster.
 HRT
HRTProgesterone for Sleep, Mood, and Perimenopause Anxiety
Estrogen gets the attention. Progesterone is the first hormone to decline, and is responsible for the 3 AM wake-ups and rising anxiety in your 40s.
 HRT
HRTPerimenopause: The Decade No One Warned You About
The 4-10 years before menopause are where the real hormonal chaos happens. Symptoms, treatment, and why this deserves more attention.
 HRT
HRTAm I in Perimenopause? The 15-Question Symptom Quiz
Interactive quiz. Score your symptoms against evidence-based criteria.
 Hormones
Hormones12 Evidence-Based Ways to Raise Testosterone Naturally
Before you consider TRT, these are the foundations. Sleep, training, nutrition, and the supplements with actual data behind them.
 Hormones
HormonesThe HPG Axis: From Hypothalamus to Gonad and Back
The HPG axis is the master regulator of reproductive hormones. Understanding the feedback loops explains why TRT, enclomiphene, and HCG produce different downstream effects.
 Hormones
HormonesDiurnal Hormone Rhythms: Cortisol, Testosterone, GH
Hormones follow daily rhythms. Cortisol peaks in the morning. Testosterone peaks at waking. GH bursts at night. Disrupting the rhythm disrupts everything downstream.
 Lab Panels
Lab PanelsCortisol Tests: AM Serum vs 4-Point Saliva
Different cortisol tests answer different questions. Pick the right one or you can miss the very pattern you're trying to see.
 Weight Loss
Weight Loss"Ozempic Face": What's Actually Happening
It's rapid-fat-loss face, not drug-specific face. The prevention strategy and what to do if it's already happened.
 Weight Loss
Weight LossWeight Loss Plateaus: Why They Happen and How to Break Through
The 7 real causes of weight loss stalls, and exactly how to restart fat loss when the scale stops moving.
 Weight Loss
Weight LossFood Noise: The Pharmacology Behind the Quiet
"Food noise" was a folk term until pharmacology validated it. Here's the molecular story behind why GLP-1 medications quiet the constant mental chatter about food.
 Longevity
LongevityThe NAD+ Salvage Pathway: How Cells Recycle Energy
NAD+ is recycled, not constantly synthesized from scratch. Understanding the salvage pathway explains why NMN and NR work as precursor supplements.
 Weight Loss
Weight LossThe Longevity Case for Losing 20% of Your Body Weight
What 20% body weight loss does for mortality, metabolic health, and quality of life, backed by SELECT and SURMOUNT data.
 Labs
LabsLDL Particle Number vs LDL-C: What's the Difference
LDL-C and LDL-P measure different things. Understanding when they diverge, and why, sharpens cardiovascular risk assessment.
 Labs
LabsFree T3 vs Free T4: Why Both Matter
T4 is the storage form. T3 is the active hormone. Both must be measured to understand thyroid function fully.
 Labs
LabsCortisol Testing: AM Serum vs Salivary Curve
AM serum cortisol is one moment. Salivary curve captures the rhythm. Each has its place in HPA evaluation.
 Men's Health
Men's HealthSleep, Testosterone, and Recovery: The Non-Negotiable Link
One bad week of sleep drops testosterone 15%. How to fix sleep first and make every other intervention work better.
 Weight Loss
Weight LossGLP-1 Receptor Biology: How These Drugs Actually Work
The GLP-1 receptor isn't just in your pancreas. It's in your brain, gut, heart, kidney, immune cells, and bone. Understanding the biology explains the body-wide effects.
 Weight Loss
Weight LossGLP-1 Receptor Desensitization: Why Effect Plateaus
After 12+ months on GLP-1 therapy, some patients notice the effect waning. The mechanism is receptor desensitization, and protocols exist to manage it.
 Hormones
HormonesAromatase: The Enzyme That Makes Estradiol
Aromatase converts testosterone to estradiol. The enzyme's regulation explains why obese men have lower T and why aromatase inhibitors can crush bone health if overused.
 Hormones
HormonesThe HPA Axis: Cortisol from Hypothalamus to Adrenal
The HPA axis controls the stress response. Chronic activation produces predictable symptoms, and understanding the system explains why fixing them requires more than "managing stress."
 Hormones
HormonesHormone Pulsatility: Why Your Body Doesn't Use Steady-State
Most hormones are released in pulses, not continuously. The pulsatile pattern carries information that steady-state delivery loses.
 Hormones
HormonesDHEA: The Precursor Cascade Mapped
DHEA is the most abundant steroid hormone in the body but underdiagnosed and underdosed. Where it sits in the cascade and why it matters.
 Hormones
Hormones5α-Reductase and DHT: The Powerful Androgen
DHT is more potent than testosterone. Understanding 5α-reductase explains hair loss, prostate biology, and why finasteride has broader effects than just hair.
 Hormones
HormonesThe Estrobolome: How Your Gut Bacteria Recycle Estrogen
Your gut bacteria determine whether estrogen gets excreted or recycled back into circulation. The estrobolome is a real and underappreciated influence on hormone biology.
 Longevity
Longevity10 Longevity Habits That Actually Have Evidence
Ranked by evidence weight. The unglamorous basics outperform every supplement stack.
 Longevity
LongevityHormone Optimization in Your 30s
The foundation decade. Baseline labs, foundation habits, fertility planning, catching early issues.
 Longevity
LongevityHormone Optimization in Your 40s
The decade where active intervention pays largest dividends. Perimenopause, low T, the window of opportunity.
 Longevity
LongevityHormone Optimization in Your 50s
Active replacement, not just optimization. Menopause, accelerating decline, and the focused playbook.
 Longevity
LongevityVO2 Max: Why It Predicts Mortality Better Than Cholesterol
One of the strongest single predictors of mortality available. Most modifiable. Almost never measured.
 Longevity
LongevityWhy Strength Beats Cardio for Longevity
Grip strength predicts mortality more reliably than cardiovascular fitness alone after middle age. The data and what it means.
 Longevity
LongevityInflammation: The Master Disruptor of Hormones and Metabolism
Most age-related conditions trace back to chronic low-grade inflammation. Understanding it as central, not as one of many issues, clarifies treatment.
 Longevity
LongevitySleep Architecture and Hormone Release: The Nightly Reset
Hormones are released in specific sleep stages. Quality sleep architecture, not just hours, drives hormonal output. Disrupting either disrupts both.
 Longevity
LongevityCircadian Biology of Hormones: The Master Rhythm
Circadian biology is the master rhythm coordinating hormones, metabolism, sleep, and immunity. Modern life disrupts it; the cost is system-wide dysfunction.
 Longevity
LongevityThe Integrated Optimization Map: Putting It All Together
Hormones, biomarkers, and lifestyle factors integrate. Optimization isn't about any single number, it's about the system. Here's the map.
 Longevity
LongevityMitochondrial Biogenesis: PGC-1α and the Engine of Aging
Mitochondrial decline drives the appearance and reality of aging. Understanding the master regulator, PGC-1α, explains why exercise is the best longevity intervention.
 Longevity
LongevitySirtuin Biology: The Longevity Genes
Sirtuins are the longevity genes, NAD+-dependent enzymes that regulate stress response, metabolism, and aging biology.
 Longevity
LongevityAutophagy and Fasting: The Cellular Cleaning
Autophagy is cellular self-cleaning, recycling damaged proteins and organelles. Fasting and exercise activate it. The benefit is cumulative.
 Longevity
LongevityCold Plunge: What's Real and What's Hype
Real effects on mood, dopamine, resilience. Overhyped claims about fat loss and testosterone. The honest breakdown.
 Longevity
LongevityResilience Markers: HRV, Resting Heart Rate, Sleep
Three daily markers that show recovery state in real time. How to interpret them and what they reveal.
 Longevity
LongevityHormone Optimization in Your 60s and Beyond
The "too old to start" framing has aged badly. Modern data supports continued optimization at any age.
 Longevity
LongevitySauna and Cold Exposure: What the Data Actually Shows
The Finnish KIHD cohort: 4+ saunas/week = 40% lower all-cause mortality. The honest evidence for sauna and cold exposure.
 Training
TrainingHow Many Days Per Week You Actually Need to Train
2 days a week is enough. 3 is the sweet spot. 4 hits 90% of the realistic ceiling. The honest math on training frequency.
 Training
TrainingBody Recomposition After 50: It's Possible
The 50s aren't too late. The protocol just looks different than at 30, and works for most adults willing to pull every lever.
 Fitness
FitnessBuilding Muscle After 40: The Complete Playbook
The physiology changes after 40. Your training and nutrition have to change too. The evidence-based guide to getting stronger at any age.
Zone 2 Cardio: The Most Underrated Longevity Training
The longevity cardio most people skip. How to find your zone 2 heart rate and why easier is often better.
 Training
TrainingThe Truth About Cardio for Fat Loss
Cardio's role is real but smaller than gym culture implies. Why volume of cardio doesn't equal fat lost.
 Training
TrainingCardio and Lifting Together: How to Combine Without Killing Gains
The interference effect is real but smaller than gym culture claims. How to program both in the same week and come out ahead.
 Training
TrainingRecomposition: Building Muscle on a Cut
"You can't build muscle and lose fat at the same time", largely false. The science of recomp and how hormones widen the window.
 Training
TrainingThe Reverse Diet: Coming Off a Cut Without Regaining
Most people regain everything within a year of stopping a diet. The structured exit ramp that prevents it.
 Training
TrainingRecovery: Why It's the Limiting Factor Most People Ignore
The real cap on body composition gains isn't training, it's recovery. Sleep, nutrition, deloads, HRV, and the signs of underrecovery.
 Training
TrainingThe Resistance Training Fundamentals Most People Skip
Five principles separate people who change their bodies from people who spin in place. Compound lifts, intensity, volume, overload, and consistency.
 Training
TrainingFull-Body Splits That Actually Work for 2 and 3 Day Weeks
The case for full-body in low-frequency weeks: programming, exercise selection, and the data that backs it as the best ROI in fitness.
 Training
TrainingPush-Pull-Legs: Why It's the Go-To 4-6 Day Split
The dominant hypertrophy split for high-frequency weeks. 6-day, 5-day, and 4-day variants with sample programs.
 Training
TrainingWhat 10 Pounds of Muscle Does to Your Metabolism
The honest math on resting calorie burn, the bigger story of insulin sensitivity, and why muscle is now an endocrine organ.
 Training
TrainingProgressive Overload: The One Principle That Actually Builds Muscle
Random workouts produce random results. Why progressive overload is the only mechanism driving long-term hypertrophy.
 Fitness
FitnessHow Walking 10,000 Steps a Day Will Change Your Life
The simplest, cheapest, most underrated habit for fat loss, longevity, stress reduction, and mental health.
 Weight Loss
Weight LossGLP-1 and Inflammation: Why hs-CRP and IL-6 Drop
Lower hs-CRP and IL-6 are among the most reproducible findings in GLP-1 trials. The mechanism is direct, not just downstream of weight loss, and explains a chunk of the cardiovascular and cogniti...
 Weight Loss
Weight LossGLP-1 and Your Lipid Panel: Triglycerides, ApoB, HDL
Lipid changes on GLP-1 therapy are favorable but specific. Triglycerides drop dramatically; LDL changes are modest; ApoB, the cleaner marker, improves substantially.
 Weight Loss
Weight LossGLP-1 and HbA1c: The 3-6 Month Trajectory
HbA1c reflects 3 months of glycemic control. GLP-1 therapy moves it dramatically, and the trajectory predicts long-term outcomes.
 Lifestyle
LifestyleWhy You Wake Up at 3 AM (and How to Stop)
Six common causes, cortisol, blood sugar, progesterone, alcohol, sleep apnea, magnesium. Identifying yours guides the fix.
 Lifestyle
LifestyleSunlight and Hormones: The Most Underrated Lever
Morning sun shapes vitamin D, cortisol, melatonin, and even testosterone. Free, simple, almost universally underused.
 Lifestyle
LifestyleCaffeine and Cortisol: The Timing Problem
The single most-underrated cortisol intervention is delaying morning coffee 90 minutes. Free, simple, evidence-supported.
 Lifestyle
LifestyleWalking 10,000 Steps: What the Evidence Actually Shows
The famous number was a 1965 marketing campaign. The actual data points to 7,000-10,000 daily as the right range.
 Lifestyle
LifestyleBurnout as a Hormonal Disorder
Burnout has a measurable hormonal signature. Lab work makes it visible, and fixable.
 Lifestyle
LifestyleStress, Cortisol, and Why Most People's Hormones Are Undermined By It
Chronic stress doesn't just feel bad, it suppresses testosterone, blunts thyroid, and drives visceral fat. The mechanisms and the fix.
 Lifestyle
LifestyleSleep, Cortisol, and Why You Can't Outwork Bad Sleep
One week of 5-hour nights drops testosterone equivalent to 10-15 years of aging. Why no protocol fully overcomes chronic short sleep, and the fix.
 Nutrition
NutritionThe Longevity Diet: What Actually Matters for Lifespan
Keto, carnivore, vegan, skip the marketing. The evidence-based diet for long, healthy life.
NutritionCreatine: The Most Researched Supplement in History
Why creatine works for muscle, brain, and longevity, and why 95% of the "risks" you've heard about don't exist.
 Nutrition
NutritionWhy "Eat Less, Move More" Misses the Point
Calories matter. So does everything else. The full picture of what the simple advice misses.
 Nutrition
NutritionMetabolism Explained: What It Actually Is and How to Influence It
The four components of TDEE, the biggest underrated lever (NEAT), and the hormones that gate metabolic rate.
 Nutrition
NutritionCan You Drink Coffee While Fasting?
Black coffee, yes for any fasting goal. Cream or sugar, that's where the answer changes.
 Nutrition
NutritionThe Fiber Gap: Why Most Adults Eat Half What They Need
Average intake: 15 g. Optimal: 30-40 g. The most under-discussed nutritional issue in U.S. adults.
 Nutrition
NutritionInsulin Sensitivity: The Master Health Marker You're Not Tracking
Why fasting insulin, not glucose, is the early warning system. How to test and improve it.
 Lab Panels
Lab PanelsThe Complete Hormone Panel: Every Test Explained
A clinician-grade walkthrough of every hormone test, what optimal looks like, and the patterns that point to a real diagnosis.
 Metabolic
MetabolicThe Glucose Variability Story: Why Spikes Matter More Than Average
Two people with the same A1C can have very different metabolic risk. CGM data revealed why.
 Metabolic
MetabolicInsulin Resistance Reversal: The Protocol That Works
Insulin resistance precedes diabetes by 8-15 years. It's also one of the most reversible conditions, when you stack the right interventions.
 Lab Panels
Lab PanelsWhy You Need Bloodwork Before Any Treatment
No labs, no plan. Why bloodwork is the foundation of every legitimate TRT, HRT, GLP-1, or peptide protocol, and what comprehensive testing actually reveals.
 Men's Health
Men's HealthMen Over 35: The Complete Health Optimization Playbook
The inflection decade. Testosterone starts dropping, recovery slows. Here's the playbook to get ahead before 40 gets harder.
 Men's Health
Men's HealthMen Over 40: Fat Loss, Muscle Gain, and Health Optimization
40 isn't too late, it's the decade doing it right matters most. Complete playbook for fat loss, muscle, and hormones.
 Labs
LabsFasting Insulin: The Most Underused Lab
Fasting insulin reveals metabolic dysfunction before glucose or HbA1c become abnormal. It's one of the most underused tests in routine care.
 Labs
LabsMagnesium: RBC vs Serum Testing
Serum magnesium is misleading, only 1% of body magnesium is in serum. RBC magnesium captures the actual cellular status.
 Hormones
HormonesThe HPT Axis: Thyroid from Hypothalamus to T3
Thyroid biology is more than TSH. Understanding the full axis, including peripheral T4-to-T3 conversion, explains why many "normal TSH" patients still feel hypothyroid.
 Nutrition
NutritionMagnesium: The Mineral Most Adults Are Quietly Deficient In
Roughly half of U.S. adults consume below the RDA. The deficiency is invisible, but quietly undermines sleep, hormones, glucose, and recovery.
 Nutrition
NutritionVitamin D: Benefits, Dosing, and Why Most People Are Deficient
40% of adults are deficient. The effect on testosterone, immunity, mood, and longevity. Optimal levels and dosing.
 Nutrition
NutritionMagnesium for Sleep: The Most Underrated Supplement
Why magnesium works for sleep, which form to take (glycinate vs citrate vs threonate), and optimal dosing.
 Lab Panels
Lab PanelsSHBG Explained: The Hormone You've Never Heard Of
SHBG controls how much of your testosterone and estrogen is biologically active, and predicts diabetes risk a decade in advance. The complete guide.
 Lab Panels
Lab PanelsThe ApoB Story: Why Cardiologists Are Abandoning LDL
ApoB directly counts atherogenic particles. The single best blood marker for cardiovascular risk, and most physicians still don't order it.
 Lab Panels
Lab PanelsInflammation Markers: hs-CRP, Homocysteine, and What to Do
Two simple labs flag chronic inflammation years before symptoms. What optimal looks like, and the protocol to bring them down.
 Labs
LabsApoB: The Real Cardiovascular Number
Standard cholesterol panels miss meaningful cardiovascular risk. ApoB measures what actually matters: the number of atherogenic particles.
 Labs
Labshs-CRP: The Inflammation Workhorse
hs-CRP is the workhorse marker of systemic inflammation. Understanding what moves it explains a lot of cardiovascular and metabolic biology.
 Labs
LabsOmega-3 Index: The Cardiovascular Marker You Can Move
Omega-3 index reflects long-term EPA + DHA status. Higher correlates with substantially reduced cardiovascular and cognitive risk.
 Labs
LabsLp(a): The Genetic Cardiovascular Risk Most People Don't Know About
Lp(a) is the most common inherited cardiovascular risk factor, and most adults have never been tested for it. Here's why that matters.
 Labs
LabsSHBG: What It Is and How to Move It
SHBG is the protein that determines how much testosterone reaches your tissues. Understanding what moves it explains many otherwise confusing lab patterns.
 Labs
LabsHDL: Why the Level Doesn't Tell the Whole Story
HDL is more nuanced than "higher is better." Function matters more than level, and very high HDL isn't always protective.
 Labs
LabsTriglyceride/HDL Ratio: The Free Insulin Resistance Marker
The triglyceride/HDL ratio is one of the cheapest, most useful cardiovascular risk markers available. It comes free with every lipid panel.
 Labs
LabsHOMA-IR: Calculating Insulin Resistance
HOMA-IR turns fasting glucose and insulin into an interpretable insulin resistance score. Simple math, useful information.
 Labs
LabsHbA1c: What the Number Actually Means
HbA1c is the workhorse glycemic marker. Understanding what it actually measures, and what it misses, sharpens interpretation.
 Labs
LabsGGT: The Metabolic Marker Most Doctors Ignore
GGT is one of the most underused liver markers. It reflects more than alcohol, including metabolic health and oxidative stress.
 Labs
LabsFerritin: When Too Low and Too High Both Matter
Ferritin should be in a sweet spot. Too low = iron deficiency. Too high = inflammation or overload. Both produce symptoms.
 Labs
LabsIron Saturation: Beyond Ferritin Alone
Iron saturation captures iron status that ferritin alone misses, particularly in inflammation states. Standard iron panels include it.
 Labs
LabsThe TSH Range Debate: Why Optimal Differs from Reference
Lab "normal" TSH ranges include many patients with subclinical hypothyroidism. Optimal is tighter than reference range suggests.
 Labs
LabsThyroid Antibodies: Catching Hashimoto's Early
Thyroid antibodies identify autoimmune thyroid disease years before TSH becomes abnormal. Standard panels often miss them.
 Labs
LabsIGF-1: The Growth Hormone Surrogate
IGF-1 is the practical marker of growth hormone status. Understanding the optimal range matters for body composition and longevity discussions.
 Labs
LabsDHEA-S as a Marker: What the Number Means
DHEA-S is the measured form of DHEA, the most abundant steroid hormone. Levels track aging and stress, and supplementation is sometimes valuable.
 Labs
LabsVitamin D: Beyond Bone Health
Vitamin D's role extends far beyond bone. Understanding the optimal range and supplementation approach.
 Labs
LabsZinc and Copper: The Ratio That Matters
Zinc and copper compete for absorption and have opposing effects. The ratio matters more than either alone.
 Labs
LabsSelenium: The Thyroid Cofactor
Selenium is the cofactor for the deiodinases that convert T4 to T3. Deficiency impairs thyroid function despite normal hormone production.
 Labs
LabsIodine Status: Goldilocks Mineral
Iodine is essential for thyroid hormone production. Both deficiency and excess can produce thyroid problems.
 Labs
LabsUric Acid: Beyond Gout
Uric acid is more than a gout marker. Elevated levels correlate with metabolic dysfunction, hypertension, and cardiovascular risk.
 Labs
LabsFibrinogen: The Clotting and Inflammation Marker
Fibrinogen reflects both clotting tendency and inflammation. Elevated levels independently predict cardiovascular events.
 Labs
LabsHomocysteine and Methylation: The Hidden Cardiovascular Marker
Homocysteine is an amino acid that should be cleared by methylation pathways. Elevated levels signal methylation problems and elevated cardiovascular risk.
 Labs
LabsReverse T3: When Inactive Conversion Dominates
Reverse T3 is the body's brake on thyroid signaling. Elevated levels signal chronic stress, illness, or metabolic dysfunction.
 Labs
LabsB12 and Methylation: Why Methylcobalamin Matters
B12 deficiency is common, often missed, and produces neurological symptoms. The form supplemented matters.